
Blog
want to take a crack at your injuries from home?
Check out our blog posts and find the topics specific to you
Topics:










The 3 most common types of knee pain in runners
Learn the most common types of knee pain in runners and why most runners never get better.
It's Dr Mark here from Base Camp.
Knee pain sucks. Straight up. Almost every runner will experience an injury at some point. The knee is the most common running-related injury runners experience.
The good news is, for most runners, it doesn't have to stop you.
Most often, running-related knee pain from 1 of 3 different causes:
The Patellofemoral joint pain (the knee cap, the muscles, and the tendons associated with it)
The Iliotibial Band pain (aka the IT Band)
Osteoarthritis (inflammation of the knee joint)
All three of these injuries have their causes and specific solutions.
Despite that, they all come down to the same thing: doing too much, too soon.
Your body wasn't prepared for the demands you placed on it.
It happens.
BUT... if you don't want to end up in REHAB PURGATORY then take them seriously.
For runners, there are three types of knee pain you need to understand.
The first is Patellofemoral Pain (PFP) in the FRONT of the knee, and the second is Iliotibial Band (ITB) Pain on the OUTSIDE of the knee.
None of them are fun.
But they don’t have to be permanent or keep you from hitting your running goals.
In fact, chances are good if you are a runner that you will experience either PFP of ITB pain at some point in your running career.
The WRONG thing to do is ignore it, keep running at the same intensity and volume, and just hope it goes away.
Let’s talk a little bit about both types of pain and your first line of defence for both of them…
1. PATELLOFEMORAL PAIN (PFP)

Patellofemoral Pain (PFP) is pain that is located on the anterior aspect of the knee (the front).
The word sounds scary, but really it just means pain related to the patella (your knee cap) and your femur (your leg bone). Often, the tendon is involved and can be one of the primary pain generators for PFP. It tends to be MUCH more common in women (2-3 times as common in fact) and can take a long time to resolve (for some stubborn cases it can last more than a year).
Pain tends to come on slowly, and may or may not be present during every run.
In my experience, runs with a lot of downhill mileage are notorious for flaring up PFP. This is likely mainly due to the way the quad muscles need to contract to stabilize the knee while travelling downhill, even at moderate grades.
One of the most common symptoms of PFP is pain with ascending and descending stairs.
2. Iliotibial Band Pain

Iliotibial Band Pain is pain that is located on the lateral aspect of the knee, where the Iliotibial Band (ITB) connects to the lower leg bone (the tibia, which is your shin bone).
Like PFP, ITB Pain tends to come on slowly, but once it comes it rarely goes away without a fight. The pain is often worse with early knee bending (when the knee is bent to about 30 degrees) and wreaks havoc on activities like cycling and downhill running.
The function of the ITB is to preserve force while we are walking or running, and stabilize the lateral knee. Pain comes on when the bursa (and fluid-filled sack) that is located deep to the ITB insertion becomes irritated.
ITB pain is often intense and debilitating.
3. Osteoarthritis (OA)

The third type of knee pain is osteoarthritis-related knee pain.
A lot of people think that running is bad for your knees and causes OA. The reality is that osteoarthritis is LESS common in recreational runners, which means that it is actually PROTECTIVE from arthritis!
The key is to get the dosage right.
If you have already had a knee injury, there is a higher chance you will develop OA and OA-related knee pain, but it is not guaranteed.
When there is degeneration, joint changes, or arthritis in the knee, your knee is more sensitive to triggering pain. But… the dosage makes the poison. Over time, you can build up your running volume and run without pain, even if you have arthritis.
WHAT TO DO ABOUT RUNNING KNEE PAIN?

THE TYPICAL CYCLE OF RUNNING INJURIES…
Unfortunately… most running injuries tend to follow this pattern:
Initial Injury from too much running volume
> Runner takes a couple of days off because of the pain
>> The pain gets better because the pain trigger (running) is absent, but because they took time off, their tissue fitness also decreased
>>> Runner returns to running at their usual pace and volume without building the tissue tolerance back up or following a progressive plan
>>>>> The runner gets injured AGAIN and starts the cycle all over.
Ready to BREAK THE CYCLE?
the better strategy:
Regardless of the type of knee pain, the approach remains pretty much the same, with some subtle tweaks.
The first step is to try and rule out something worse PFP or ITB Pain which are both ‘non-complex’ biomechanical conditions. We want to make sure it isn’t something more severe like a bone-stress injury (stress fracture), connective tissue injury like a meniscus tear or ligament damage, or infection/disease-related. We can’t always rule these things out, but we try and be as confident as possible that the pain is in fact something we can deal with conservatively (without drugs/injections or surgery).
Don’t misinterpret the above information though. Just because something isn’t ‘medically’ serious, doesn’t mean the pain isn’t severe or debilitating.
IF the pain does in fact fall into the category of either PFP or ITB Pain, we take a 3-step approach to managing, fixing, and preventing the condition from coming back.
Step 1: CALM STUFF DOWN
Step 2: BUILD BACK UP
Step 3: BRIDGE THE GAP
Step 1: CalM Stuff Down
The first thing we need to do with either knee pain condition is to calm down the pain so you can get back to running without making things worse.
Our first line of defence is some DELOAD work. This means taking a few days or weeks off. No runner likes to hear this. But some sort of deload is essential for calming the pain down. For some runners, that does not mean COMPLETELY stopping running. We try really hard to keep runners running, because we know one thing is true: RUNNERS LIKE TO RUN.
Step 2: Build Back Up
Once the pain has calmed down a bit, then we move into our Build phase. This focuses on building your strength, endurance, and tissue tolerance back up to handle the demands of running. This usually looks like some strength and cardio training BELOW symptom threshold.
Step 3: Bridge the Gap
Once we have built the tissue tolerance back up, we need to bridge the gap from rehab back to performance. Just because the tissue is strong, does not mean it is necessarily ready for the demands of the running you were doing before injury.
This process is collaborative and involves some trial and error. Too much too soon? We take two steps backwards.
While it is tempting to jump right back into your regular running routine because you are feeling so much better, it is a much better idea to gradually build your running volume back up.
Ok… but what does that actually LOOK like?
Fair question, that I wish I had a straightforward answer to. Unfortunately, everyone is different. There is no single exercise, stretch, or rehab plan that works for everyone.
If your knee pain is keeping you from running, or doing anything else you love, I HIGHLY recommend you seek out a qualified provider.
That said, if you want to take a shot at fixing your pain yourself from home, here are some of the exercises I often use with my patients.
PFP EXERCISES:
Tempo Squats (3-seconds down, 1-second hold, 1-second up, 0-second rest at the top)
Rear Foot Elevated Split Squats
ITB Pain Exercises
Stationary Cycling (with your knee flexed to about 35 degrees at the bottom of the stroke. Move your seat forward and down to accomplish this).
Uphill Treadmill Walking (8-10 degrees incline)
Rear Foot Elevated Split Squats
Want 1-on-1, personalised rehab?

Author: Dr Mark Murdoch, Chiropractor and Co-Founder at Base Camp Chiropractic and Sports Rehab in Vernon, BC.
Mark Murdoch is a Doctor of Chiropractic with a Master’s Degree in Sports Medicine.
Contact: drmurdoch@basecampclinic.com
Instagram: Base.Camp.Doc

How long does it take for Achilles tendonitis to heal? (updated 2024!)
Achilles Tendon pain can be super frustrating. Learn how long it might take you to recover

Achilles Tendon pain can be INCREDIBLY frustrating.
This is especially true if you can’t participate in your activities of choice because of the pain. I often see Achilles Tendinopathy in runners, hikers, volleyball players… It sucks for everyone.
The most common question I get when someone comes in with Achilles Tendon pain is “how long is this going to take?”
This is not my favourite question to answer, because Achilles Tendon pain can last a LONG TIME.
The short answer to that question is “1-12 months”, but that doesn’t really help anyone. The slightly longer answer to that question is “it depends”, which ALSO is not very helpful…
In order to estimate your recovery time, you need to understand two things:
Severity and Stage of your injury
Other factors that influence your performance
Let’s break it down a little bit, and you can see where you might fall in the estimated recovery time.

Stop letting Achilles pain slow you down!
Get started with our client success guide.
Where does it come from?
Why does it come back?
How to do a self-assessment at home
Recovery expectations
and more!
Grading the Severity and Stage of your Injury
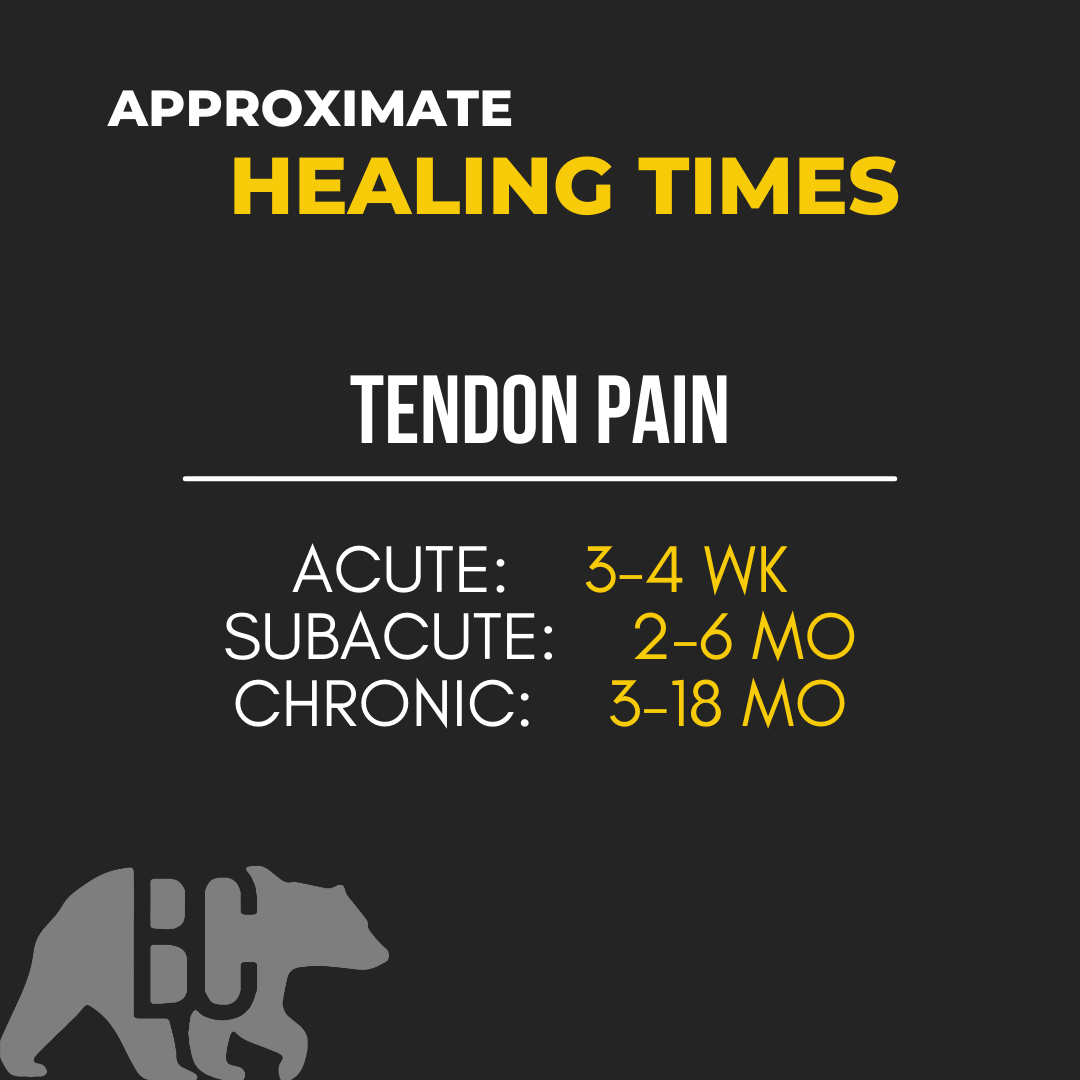
Achilles Tendinopathy falls into 3 Stages:
Acute (new onset of pain, up to 2 weeks)
Subacute (immediately after acute, 3 weeks-2 months
Chronic (3 months plus)
The later longer it has been since the onset of injury, the longer it generally takes to recover.
Acute Achilles Tendinitis will usually calm down in 3-4 weeks (I say CALM DOWN, not GET BETTER here. This is explained later in this article under the header ‘Calmed Down vs Gotten Better).
Subacute Achilles Tendinopathy will usually take 2-6 months to calm down. (Again, not better yet)
Chronic Achilles Tendinopathy is a tricky one and can take anywhere from 3 months to 18 months to calm down and get better.
FACTORS THAT INFLUENCE RECOVERY TIME
This list is a long one, so I will only list the ones I feel are most important. These include:

Overall Health
Crappy Diet? Super stressed out? Smoker? Comorbidities like diabetes, metabolic syndrome or heart disease? All of these things lengthen the expected recovery time.
Mindset
Positive mindsets win the rehab game.
Sleep
You can’t out rehab 5hrs per night of sleep, especially while trying to recover from an injury. You NEED 8hrs + of sleep per night if you want to get better in a reasonable time and keep the injury from coming back.
Rehab Plan
Your rehab plan needs to be well-thought-out, progressive, and appropriate to both your current state and the activities you want to get back to. If you are a runner and your rehab plan does not involve running at some point, you are following the wrong plan. Volleyball? You better be jumping at some point in your plan. (But not too much too soon…)
Calm Down vs Get Better
This happens time and time again. Someone comes to see me and together we are able to get them out of pain, and they feel better, so they decide to cancel their follow up and get back to their activity.
Inevitably, a couple of weeks later they are back in my office, 2-steps back.
This is because their injury was not fully rehabbed. Only their PAIN is better, but they have not been fully prepared to get back into their activity at 100%. This takes time, deliberate effort, and a well-thought-out progressive rehab plan.
Moral of the story: just because the pain goes away, does not mean that you are ‘better’ (especially true with Tendon injuries).
Rehab programs should generally have 3 Steps.
Step 1: RESET - Calm Stuff Down
Step 2: Restore - Build Back Up
Step 3: Reload - Bridge the Gap
MOST rehab plans end after calming stuff down. SOME plans do a decent job of building strength and endurance back up. VERY FEW programs bridge the gap between recovering from an injury and performing the way you want to.
Need some help?
That is where we come in. If you are ready to get on a plan that will get you back in action and back to doing the things you love, and KEEP THIS INJURY FROM COMING BACK, we can help.
Author: Dr Mark Murdoch, Chiropractor and Co-Founder at Base Camp Sport and Spine in Vernon, BC.
Mark Murdoch is a Doctor of Chiropractic with a Master’s Degree in Sports Medicine.
Contact: drmurdoch@basecampclinic.com
Book an Appointment with Dr Murdoch: book here
Instagram: Base.Camp.Doc
Achilles Tendinopathy (UPDATED 2024!)
One of the most common running injuries, Achilles tendon pain can sideline you for months. If you think you might have Achilles tendinopahty, make an appointment today so we can get you back to doing what you love.
In this article:
what is Achilles tendinopathy
Who gets Achilles tendinopathy
How we diagnose Achilles tendinopathy
What to do if you have Achilles tendinopathy
It goes a little something like this…
You’re new to running and decided that trail running is for you (YES! Stoked for you). The runs so far have been pretty enjoyable, but you are ready for something a little bit more challenging than the Rail Trail. This week you are ready to put some miles in at Kal Park! Can’t be that hard right?
So you pick up a brand new pair of Trail Runners, pick a trail and start moving.
It went great! You had such a blast. The VIEWS! They were just amazing. Sure, the hills were hard, but that’s good for you, right? Nothing like a little uphill challenge.
The next couple of weeks go great. Instead of road running, you are strictly on the trail and instead of the measly Rail Trail, you are strictly running the rolling hills of the North Okanagan.
One day while running your new favourite Kal Lake route you start to feel some discomfort in your lower leg. It’s on the backside, a couple of inches up from your heel. That’s weird. This has never happened before. It’s not a big deal though. After a km or so it goes away and for the rest of the run you don’t even feel it. “It must have been nothing”, you think.
But the trend continues… next week you are feeling the same pain on every run and it’s starting to last longer. It doesn’t quite go away by the end of your run. Instead, it keeps getting worse! After your run it calms down, but lingers for a few hours. “This must just be part of becoming a runner. I just have to deal with some pain sometimes”.
The next morning you step out of bed and OUCH. Your Achilles HURTS! It’s a tension/burning/shearing pain. It hurts to stand and it hurts to walk.
What the heck is going on?
ANSWER:
A good ol’ case of Achilles Tendinopathy.
What is it?
Achilles Tendinopathy is a really common overuse running injury. As many as 85% of middle-distance runners will experience it.
The Achilles is a tendon that attaches your calf muscle (back of your lower leg) to your foot. It attaches to the top of the back of your heel and is one of the main ways we transfer force through our feet while running and walking. When we start to get Achilles pain it can start to affect EVERYTHING YOU DO throughout your day. It sucks, but most people recover from it with proper treatment and rehab.
Tendinopathy is a fancy word to describe an inflammatory and remodelling response process that happens when the Achilles tendon is overloaded and is unable to recover. The catch is that it will often get worse if it is just ignored. Early recognition and intervention are key in shortening the recovery time.
A typical case of Achilles tendinopathy starts slow and becomes more severe over time until it is present every time the tendon is loaded.
Who gets it?
While Achilles Tendinopathy seems like it should be more prevalent in competitive athletes, 65% of cases are from the general public and are not sport-related.
There are a few risk factors that increase your chance of getting Achilles Tendinopathy that I divide into 2 categories: things you CAN control and things you CANNOT control
Things you CAN control:
Ankle strength (weak ankles, especially with pressing your toes down, is a risk factor)
Sudden changes in training volume (too much, too soon)
Uphill running (if you are unprepared for it)
Fluoroquinolone antibiotic use (e.g. ciprofloxacin) has been shown to significantly increase the risk of tendon injuries (not just Achilles tendon!). If you are on antibiotics, it is wise to change your training program temporarily. Talk to your prescribing doctor if you are unsure about the type of antibiotics you are taking and if there are alternatives
***Increased body weight and abnormal ankle range of motion. While these aren’t always completely within our control, a little change can go a long way. You don’t need to have perfect range of motion or body composition to avoid Achilles tendinopathy
Things you CANNOT control:
Family history of tendon injuries
Genetic variation
Systemic disease
Abnormal ankle range of motion.** (If you have a previous injury that limits your range of motion or have hypermobility, your ROM might be out of your control).
How does a doctor diagnose Achilles tendinopathy?
As a Chiropractor in Vernon, BC, who sees a lot of sports-related injuries, I use a two-stage process to diagnose Achilles Tendinopathy
Step 1: History
During the history portion, I ask a ton of questions to determine if Achilles tendinopathy is responsible for your symptoms.
There are some typical things we hear in the history that tip me off as a Sports Medicine practitioner:
Pain at the Achilles tendon, either in the middle of the tendon, the heel, or the tendon-muscle junction
Pain that has progressed over time and gotten worse with activity
Engaging in a running, walking, or pedalling activity
Previous history of tendon pain or injury
Other aspects of a patient history I look for when a patient comes in with Achilles pain:
Antibiotic use (certain antibiotics increase the risk of tendon injuries)
Recent increases in training volume
Changes in training terrain (especially adding hills to a running program)
Changes in running footwear
Family history of tendon injuries
Systemic diseases
Other life stressors
Step 2: Physical Exam
During the physical exam, I test out your joints, muscles and tendons, check your range of motion, and strength, and perform some other tests to determine the cause of your pain, the severity of your injury, and your current limitations.
Here are some things I typically look for on a physical exam for Achilles tendinopathy:
Pain with pressure (usually a pinch) on the Achilles Tendon
Pain with loading the tendon (pressing your foot down, like a Calf Raise)
Thickening of the tendon or nodules on the tendon
Redness or swelling along the tendon
Endurance of the calf musculature
Ankle, knee, and hip range of motion
Strength of the ankle and knee
Check your gait (running and walking)
What to do when you have it?
One of the most important things to do if suspect tendinopathy is to NOT WAIT to get an assessment, get treatment, or change your training. The worse a tendinopathy gets, the longer it can take to heal.
Here is what the typical process looks like:
STEP 1: Get Assessed.
STEP 2: Get A Plan.
STEP 3: Get Better.
Achilles tendinopathy does not always mean you need to completely stop your activity, but a period of relative rest is essential. In order to heal we need to decrease the demands on the tendon to a level that you can recover from.
If you suspect you have Achilles tendinopathy, take a couple of days off of your primary activity (for this example we will use running) and see how your body responds. If you notice your pain is going down, it is wise to take a week or two off and then try a short slow run.
In my treatment room, the first thing I use to treat Achilles pain is a combination of manual therapy and exercise to manage pain. Once the symptoms start to calm down, we start building your strength and endurance back up. After a period of strength training, we slowly build back up to running.
How to treat your Achilles Tendinopathy from home:
**NOTE: Achilles tendinopathy is not something I recommend most patients manage by themselves. Having a clinician to help guide you improve your chance of success and decreases your chance of re-aggravation.
Treatment follows 3 Steps: 1) Calm it Down, 2) Build if Back Up, 3) Get Back to Activity
Phase 1: Calm it Down
ISOMETRICS (Weeks 1-2)
The first thing we want to do is manage your symptoms. This is especially important if you have any swelling.
Relative Rest/Deload: take 2-3 days off of your activity and see how you respond. If you are worried about your running fitness, try switching it up for cycling, rowing, swimming, or circuit work that does not include running or skipping
Self-Myofascial Work/Foam rolling: this can give some temporary relief for the calf and ankle. Avoid rolling out directly on top of the painful tendon
Isometrics: isometrics are exercises that load the muscle and the tendon but simultaneously provide a pain-relieving effect. I typically recommend my Achilles tendon patients use some variation of this home exercise prescription:
Phase 2: Build it Back Up
The next phase of Achilles tendinopathy rehab is to build your strength and endurance back up. I use eccentric exercises first and then progress into concentric exercises.
ECCENTRICS (Weeks 2-5)
Eccentrics allow us to load the calf and its tendon in a way that is highly controlled. The key to using Eccentrics here is tempo, and not moving too quickly throughout the exercise.
At the start of Week 3, if symptoms have calmed down, re-introduce a short, slow run just to gauge how your recovery is going. When I say short I mean SHORT. 400-1000 m is enough. If you tolerated it well (mild pain during the run, and lingering pain that does not last more than 24 hours) then you can start running that distance ONCE per week.
FULL RANGE OF MOTION (Weeks 6-9)
Using the full range of motion of the ankle puts the muscle through each type of contraction. The only reason I use concentric exercise AFTER eccentric exercise is that for many patients it is easier to control in this order.
We progress each exercise from both feet to one foot as tolerated to prepare the tendon to handle your full body weight.
At the start of Week 5, re-introduce up to 30% of your typical running distance for the next two weeks (e.g. if you run 10km in a week, limit yourself to 3km for Weeks 5 and 6)
At the start of Week 7, re-introduce up to 50% of your typical running distance for the next two weeks (e.g. if you run 10km in a week, limit yourself to 5km for Weeks 7 and 8)
Phase 3: Get Back to Activity
This is where we start to risk re-aggravation. While some pain is normal and acceptable with tendon rehab, we don’t want to go backwards, but we also want to push your limitations so that we know you are closer to getting back to your activity at as close to 100% as possible.
BALLISTICS (Weeks 10-12)
Ballistic exercises (hopping, skipping, running, etc.) load the tendon rapidly and take advantage of its elastic properties (one of the main functions of the tendon). The tricky part here is that it is the elastic nature of the tendon that causes the damage in the first place (the elastic was overstretched too many times before it could heal). This is why a gradual introduction of ballistic exercise is essential. It is best to progress slowly.
How long does it take to recover?
I would like to apologize in advance for this next part. Firstly, because you are not going to like and answer, and secondly because there really ISN’T a concrete answer.
Like most injuries, Achilles tendinopathy recovery varies from person to person, but if left untreated it can take UP TO A YEAR to recover. Oof.
That said, not everyone will take so long to recover. How quickly you recover will depend on a few things such as:
How quickly you recognize there is a problem and change what you are doing. Early recognition and then intervention leads to faster recovery because we can start treatment and rehab BEFORE the injury becomes severe.
Have you had tendinopathy in the past? This may take longer to heal
Are you currently on antibiotics? This one is a tricky one (caveat: I am not a medical doctor, and you should always consult your prescribing doctor before messing with your medication), but sometimes can be super simple. In some cases, simply finishing your antibiotics course or changing antibiotics is all it takes.
Do you have optimal ankle ROM? If you have limited range of motion, work to improve it. If you have excess range of motion, work on ankle strengthening
What is your overall health? Stress level? Improving other areas of your life can improve your ability to heal from injury.
Should I stop running?
Ahhh, here we go. The real reason you are here. Should I stop running with Achilles tendinopathy? This is, again, a super complex question. Kind of like “should I buy a house?” or “should I get face a tattoo?”. There are going to be different answers for every person who asks the question, and context is essential to making the right decision.
In many cases of Achilles tendinopathy, a period of relative rest IS essential to the healing process. Unlike other injuries, tendinopathy is hard to work around and keep running.
That said, there are some strategies to keep you running. If you need to keep running, here are some modifications that can be helpful:
Avoid uphill running
For a period of time, shorten your runs. Start with 50% of your normal distance and see how you feel.
Find a shoe with a higher drop (the difference between your heel and your forefoot). This can help take some of the stress off your Achilles while you are rehabbing.
GET ON IT EARLY. The earlier you recognize you may have Achilles tendinopathy the better your chances of a quick recovery.
Start rehab and see how you feel. I try and keep as many of my patients running as possible, even while they continue to rehab their Achilles
How to avoid it
Simple. All you need to do is manage all of the stressors in your life, get enough sleep, and never train more than you can recover from, and eat a perfect diet.
Ok… maybe not as easy as it sounds.
Unfortunately, controlling all of the variables involved in order to avoid Achilles Tendinopathy is not always possible. BUT there are at least a few things you can do.
IMPORTANT NOTE: just because you can’t do ALL of these tips, does not mean that doing SOME of them is not helpful. Pick one or two and focus on getting them right, then add in the others later.
SLEEP
Aim for 8+ hours of sleep per night. There is NOTHING more protective from injury than sleep.
NUTRITION
Get enough protein (1.1-2.5 grams of protein per kg of body weight per day) from as many whole sources (animal sources) as possible. Getting enough can be hard, so don’t be afraid to supplement with a protein shake if needed.
STRENGTH
Resistance train (lift weights) 1-3 times per week. Specifically for Achilles pain, heavy calf raises with your knee straight and again with your knee bent is really helpful.
MANAGE YOUR STRESS
If you are mega stressed out, your injury risk goes up. Consider using mediation, yoga, breathwork, or other relaxing methods to manage your stress.
MANAGE YOUR TRAINING
Too much, too soon. If you are new to running, don’t be afraid to take it slow. This recommendation is doubly relevant if you aren’t managing any of the other aspects of injury.
GET CHECKED
Think you might have Achilles Tendinopathy? Get checked. Don’t let it get so bad that you have to sideline your training.
Author: Dr Mark Murdoch, Chiropractor and Co-Founder at Base Camp Chiropractic and Sports Rehab in Vernon, BC.
Mark Murdoch is a Doctor of Chiropractic with a Master’s Degree in Sports Medicine.
Contact: drmurdoch@basecampclinic.com
Instagram: Base.Camp.Doc
Disclaimer: This blog is intended for general informational purposes only and is not intended for the delivery of medical advice. No doctor/patient relationship is formed. The use of information on this blog or materials linked from this blog is at the user's own risk. The content of this blog and website is not intended to be a substitute for medical advice.

Running with lower back pain
‘Don’t do that, it’s bad for your back’
Have you ever been told that?
What if I told you… running is good for you?
Lower back pain is one of the most common injuries out there. As many as 8/10 people will have lower back pain in their lifetime.
That is practically everyone!
There are a lot of runners who have lower back pain. You probably even know some. But… what if I told you that running is not only safe for your lower back, it may even be protective???
Let’s look at why…
How common is Lower Back Pain?
Lower back pain is EXTREMELY common. I guarantee you either have lower back pain or know someone who does (PSA: if you don’t know anyone with lower back pain, you might want to work only our listening skills).
It affects 35-80% of people at some point in their lives, and as many as 50% of people with lower back pain with have chronic pain (multiple episodes of lower back pain), at a conservative estimate.
So then… common is lower back pain in runners?
On the generous side: 22% of runners will develop lower back pain. On the more optimistic estimate? as low as 1% of runners have lower back pain 🤯
By those numbers… that means that running is likely PROTECTIVE for your lower back, instead of bad for it!
Now… all pain is multifactorial. That means that a lot of things can contribute to your pain experience (sleep, stress, nutrition, family history/genetics, previous injury… you get the idea).
But physical activity and being overall healthy are likely protective against most types of pain. By that rationale, running is not only good for your overall physical and mental health, but it can also decrease your chances of developing lower back pain.
In other words, if you are thinking about starting to run or you’re a current runner and worried about running making your back pain worse, you have my permission to stop stressing about it.
Get you there and put some miles on those shiny new shoes!

But what if I already have lower back pain from running?
It happens. As we talked about above, your lower back pain likely is not CAUSED by running, but it may be aggravating to it.
The first thing I recommend is getting assessed by a clinician you trust (preferably one who works with a lot of runners). If you need some help, we are here. Start with a free consult and we will help point you in the right direction.
There are a few reasons why you might have lower back pain and why running might make it more irritated.
Here are some common causes of lower back pain among runners:
Lower back or SI joint irritation
Lower back muscle strain or muscle pain
Lower back disc irritation that gets worse with running
Poor hip, ankle, or knee function
Other things in life can also contribute to back pain, that don’t even have anything to do with running like:
Stress
Poor sleep
Inadequate nutrition or hydration
History of injury
Other conditions like obesity, diabetes, or metabolic diseases
Lower back pain is complex. It is probably the most complex condition that walks into my door. That is because human beings are complex. You aren’t just a runner. You are also a mom, an uncle, a boss, a volunteer, etc. All of the other parts of life contribute to your pain experience, and we can’t just isolate ‘the SI joint’ or arthritis as the sole cause of your symptoms.
With that said… let’s talk about some things you can work on to HELP with your lower back pain (even if they aren’t necessarily the sole cause).
what to do if you have lower back pain with running
If you ARE having lower back pain and running makes it worse, here are a few things we work on at our clinic to fix low back pain with running:
Hip Mobility
Core Strength
Ankle Mobility
Hip Strength
1) Hip Mobility
Improving your hip mobility can improve your ability to access your hips, and give the lower back a break. Try this stretch and exercise:
90/90 and Shin Box
2) Core strength
Side Bridge is probably the exercise that I give most often to runners. I consider it something of a panacea for most running pain and injuries. If your core endurance and strength is poor, your form will break down sooner. This can lead to earlier irritation of the lower back (or knee… or hip… or ankle…)
I recommend that all runners be able to hold this for at least 60 seconds, but 25 km+ runners hold it for 90 seconds and ultra and marathon to runners hold it for 2 mins easily
Here is hot to test your side bridge endurance:
3) ankle mobility
The body is connected, from the big toe to the base of the skull. Somethings working on your ankle mobility can improve function upstream (e.g. at the hips or lower back)
Here is how to assess your ankle mobility and a good ankle mobility exercise:
4) Hip strength
Not surprisingly, hip strength is VERY important for runners.
Here are two exercises I give my running clients and patients all the time
At the end of the day, there are many reasons you might have lower back pain with running.
If you want more guidance, we can help.
Start with a free consult and learn more about our custom Pain to Performance plans and our Super Runner program, to get you back to running unlimited by low back pain.
Author: Dr Mark Murdoch, Chiropractor and Co-Founder at Base Camp Sport and Spine in Vernon, BC.
Mark Murdoch is a Doctor of Chiropractic with a Master’s Degree in Sports Medicine.
Contact: drmurdoch@basecampclinic.com
Instagram: Base.Camp.Doc

Heel Pain in Runners
Heel pain in runners is common. It is especially prevalent in new runners, experienced runners getting back into running, and runners who have started a new program or increased their running volume.
If you are experiencing heel pain, I don’t have to tell you how frustrating and painful it can be. It often sidelines runners and is rarely a quick fix.
Here are some things you should know about heel pain in runners and how we approach heel pain here at our sports rehab clinic, Base Camp Chiropractic in Vernon.
Types/Causes of Heel Pain
Heel pain commonly comes from 3 or 4 different sources.
Plantar fasciitis

If you are a runner and haven’t heard of plantar fasciitis, you have clearly been spending too much time with your headphones in, because I guarantee someone you know has it or has experienced it.
Plantar fasciitis is when the fascia (connective tissue that supports your arch) is over-stressed and becomes inflamed and irritated. It is typically worst in the morning and while you are running. The onset is often sudden, and you just wake up one day with heel pain.
You can test your plantar fascia by pressing on point 1 (in the picture) and passively extending your big toe with your other hand. If this is extremely painful, there is a chance you have plantar fasciitis.
To deal with this, try this stretch every morning: Plantar Fascia Stretch
… and check out this article on foot strengthening exercises: Foot Strength for Runners
You can also try things like orthotics or a heel lift to change the load on your heel as a temporary change to deload the irritated tissues.
Achilles tendonitis
Achilles tendonitis is common in runners who have started to introduce a lot of uphill running. The Achilles tendon becomes overloaded and irritated, and can no longer recover from your running. Pain can be located along the calf, between the muscle and the heel. For some people, that pain can radiate down to the bottom of the heel and foot as well.
To work on this, you need to work on your calf strength and ankle range of motion.
Start working on your calf using calf raises. If calf raises are painful, you can limit your range of motion to start (see the video below).
You can also work on calming down your calf muscle tone by using foam rolling and the 3-direction ankle mobilization (the other videos below).
You can also try things like orthotics or a heel lift to change the load on your heel as a temporary change to deload the irritated tissues. I often recommend limiting your uphill running when the Achilles is really irritated. In general, shoes with a larger drop (an elevated heel relative to the ball of the foot) will decrease your chance of developing Achilles pain and improve symptoms.
Stress fracture
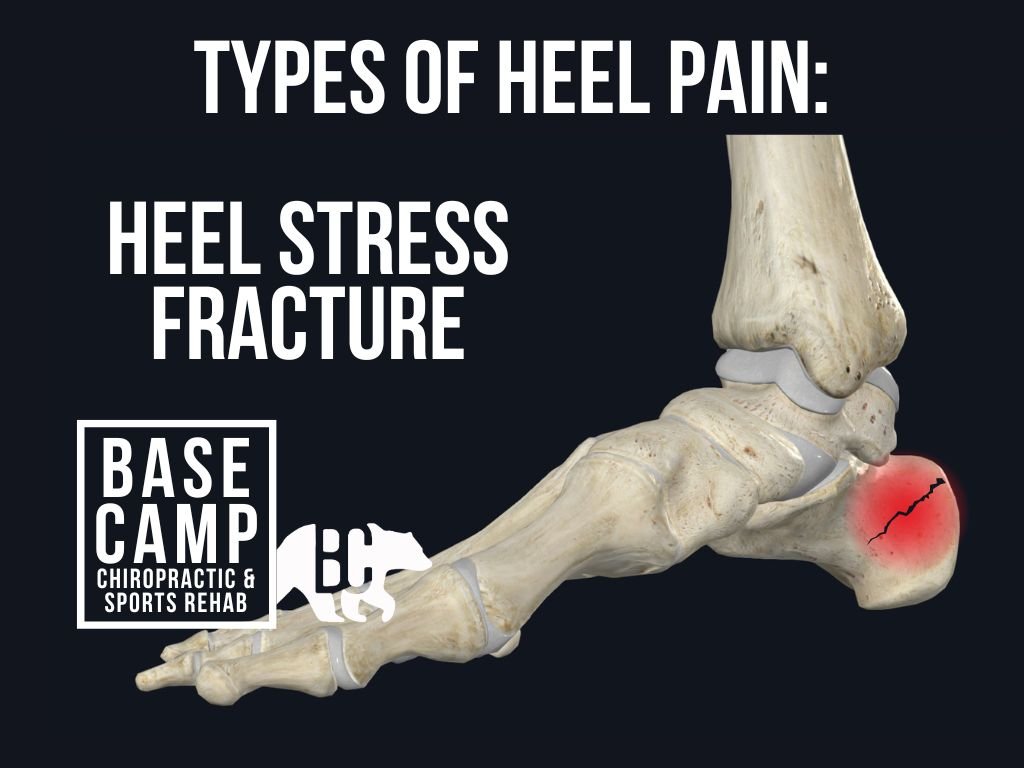
Stress fractures happen when the stress we have put the bone through is more than it can recover from. These injuries happen over time.
There is only one solution to stress fractures: rest.
Unfortunately, if a stress fracture is the cause of your symptoms, then you have to stop running for a few weeks and wear an air cast until the bone has healed.
Stress fractures are often very tender to the touch, you may have redness or swelling, and trouble running or walking at all.
If you think you might have a stress fracture, you need to go see a chiropractor, physician, or physiotherapist in Vernon who works with runners.
Sciatic nerve
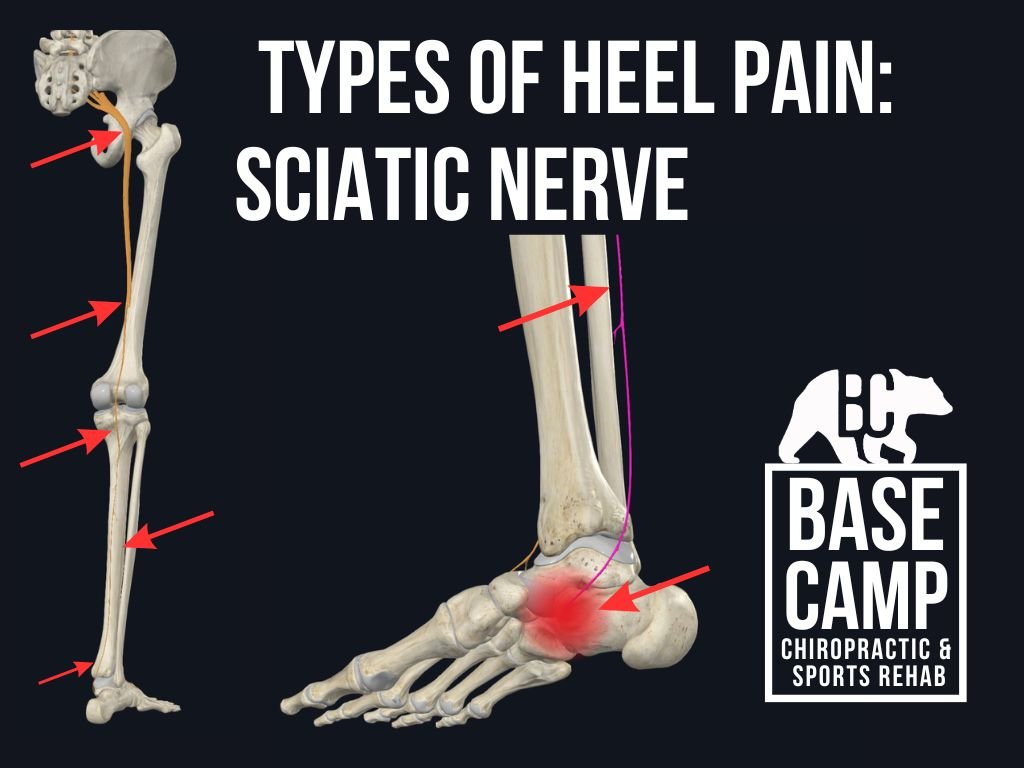
I see a lot of cases of heel and foot pain that have been diagnosed as ‘plantar fasciitis’ when in reality the problem is coming from the lower back. The sciatic nerve starts in the lower back and goes down to the bottom of the foot. In this case, the foot is not the primary culprit, even though the symptoms are in the foot.
TRY THIS STRETCH:
If this stretch makes your foot BETTER then we can be pretty confident that the lower back is involved. If this is the case, it is worth getting assessed by a physiotherapist or chiropractor in Vernon who can help you work on the lower back and whatever might be causing the symptoms.
(PSA: it is NOT because your pelvis or hips are out).
Don’t let your pain or injuries hold your back. Book a free consult with Dr Mark to get you back on the trails and stay injury free this running season.
Author: Dr Mark Murdoch, Chiropractor and Co-Founder at Base Camp Sport and Spine in Vernon, BC.
Mark Murdoch is a Doctor of Chiropractic with a Master’s Degree in Sports Medicine.
Contact: drmurdoch@basecampclinic.com
Instagram: Base.Camp.Doc
How running injuries happen